This study aimed to better understand the effectiveness of the Ertl transtibial amputation and to learn more about the mechanics of sit-to-stand and stand-to-sit transitions. To do so, we studied the differences in joint angles of the ankle, knee, and hip and the excursion in center of pressure in both the x and y range between an Etrl amputee (both intact and amputated limbs) and a control subject during STS tasks. Our results showed significant differences in the minimum knee angle, minimum ankle angle, maximum ankle angle, ankle range of motion, excursion in the x range, and excursion in the y range.
Hip
The lack of significant difference found at the hip joint suggest that the Ertl amputation is effective in allowing a transtibial amputee to return to relatively natural range and use of the hip joint during STS transitions.
Ankle
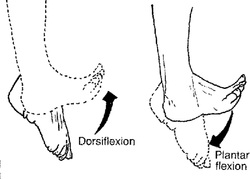
In contrast, the large amount of significant differences found surrounding the ankle joint suggest that the Ertl amputation is not effective in allowing amputees a relatively normal use of the ankle joint during STS transitions. Furthermore, because subjects’ feet placement was not regulated as long as each foot was on a force plate, the negative minimum ankle angles shown in the intact and amputated limbs of the amputees may suggest that amputees use a different strategy when sitting down, and may be seated with the ankle remaining in plantar flexion. There is also a larger standard deviation seen in the ankle joints of amputees relative to the standard deviation of control subjects. This suggests various possibilities. This may suggest that healthy control subjects have a consistent and reliable pattern for making a STS transition which is congruous with findings of Agrawal et al. (2010), showing a consistent STS transition pattern in healthy controls. Similarly, this may suggest that amputees have varying and inconsistent strategies for making STS transitions. These larger standard deviations in ankle joints of amputees may also suggest a range in the confidence levels of amputees about making STS transitions. The various significant differences in the ankle joints of the amputated leg may also be explained by the functional unease of the prosthetic ankle joint. Due to the fact that the prosthetic ankle does not undergo plantar flexion or dorsiflexion as easily as a true ankle joint, amputees are forced to rely more heavily on bending the prosthetic foot rather than dorsiflexion of the ankle. This helps to explain why the ankle range of motion of the amputated limb significantly differs from that of the intact limb and from that of the control limb. This also helps to explain the lack of significant difference between the intact limb and the control limb.
knee
Furthermore, the reliance of foot flexion rather than dorsiflexion of the ankle translates into explaining the significant difference found in the knee minimum angle between the amputated limb and the control limb. This difference suggests that because amputees come further forward onto their toes during STS transitions, they fail to completely straighten the knee on the side of their amputation. This also helps to explain the lack of significant difference seen in the minimum knee angle of the intact limb.
Center of pressure
Lack of ankle range of motion in amputees may also suggest an explanation for the significant differences seen in X range center of pressure excursion. Due to the fact that amputees do not have the functional mobility in a prosthetic ankle joint as compared to an intact ankle joint and therefore must bend the foot rather than dorsiflex the ankle, it is only natural that center of pressure must shift forward when the amputees come forward onto their toes. This significant difference between the amputated and control limb are seen in both sitting and standing transitions and may suggest that pressure in the amputated limb stays toward the toes during the entire standing period. There was also a significant difference seen in y range center of pressure excursion between the amputated and control limb. This indicates a shift in the center of pressure of towards the left or right in the amputated limb compared to the control limb; however, it is unclear in which direction the shift occurred because these data were not analyzed. Although there was shown to be a significant difference in the Y range excursion between the amputated and control limb, this difference may not show to be as physiologically significant as the difference seen in the X range excursion. The Y excursion was less than a centimeter which may not be physiologically significant. In contrast, the X range shift was much larger and therefore should theoretically cause a larger risk of traveling outside the base of support, leading to a greater risk of an extra step or of falling.
